Sat, Jul 12, 2025
| فارسی
Volume 23, Issue 1 (Spring 2017)
IJPCP 2017, 23(1): 38-49 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dasarband B, Panaghi L, Mootabi F. Relationship Between Spouse Abuse and Depressive Symptoms in Women: The Moderating Role of Personality Characteristics. IJPCP 2017; 23 (1) :38-49
URL: http://ijpcp.iums.ac.ir/article-1-2485-en.html
URL: http://ijpcp.iums.ac.ir/article-1-2485-en.html


1- Family Research Center, Shahid Beheshti University
2- Family Research Center, Shahid Beheshti University ,Email: l-panaghi@sbu.ac.ir
2- Family Research Center, Shahid Beheshti University ,
Full-Text [PDF 2058 kb]
(3568 Downloads)
| Abstract (HTML) (8075 Views)








References
[1]Kalaca S, Dundar P. Violence against women: The perspective of academic women. BMC Public Health. 2010; 10(1):490. doi: 10.1186/1471-2458-10-490
[2]Meier JS. Brief of the domestic violence legal empowerment and appeals project, aequitas: The prosecutors’ resource on violence against women, & futures without violence as Amici Curiae in support of respondent, Voisine v (Report). Report No. 14-10154. Washington D. C.: GW Law Faculty Publication; 2016.
[3]Tjaden PG, Thoennes N. Extent, nature, and consequences of intimate partner violence: Findings from the National Violence Against Women Survey. Washington D. C.: National Institute of Justice; 2000.
[4]Krantz G, van Phuong T, Larsson V, Thuan NT, Ringsberg KC. Intimate partner violence: Forms, consequences and preparedness to act as perceived by healthcare staff and district and community leaders in a rural district in northern Vietnam. Public Health. 2005; 119(11):1048-55. doi: 10.1016/j.puhe.2005.03.015
[5]Walker LE. Psychology and domestic violence around the world. American Psychologist. 1999; 54(1):21-29. doi: 10.1037//0003-066x.54.1.21
[6]Amoakohene MI. Violence against women in Ghana: A look at women’s perceptions and review of policy and social responses. Social Science & Medicine. 2004; 59(11):2373-85. doi: 10.1016/j.socscimed.2004.04.001
[7]Women‘s Research and Studies Center. Preventing Violence against women and children: Workshop summary. New York: National Academies Press; 2001.
[8]Abbott J, Johnson R, Koziol-McLain J, Lowenstein SR. Domestic violence against women: Incidence and prevalence in an emerg ency department population. Journal of the American Medical Association. 1995; 273(22):1763-7. doi: 10.1001/jama.273.22.1763
[9]Campbell JC, Lewandowski LA. Mental and physical health effects of intimate partner violence on women and children. Psychiatric Clinics of North America. 1997; 20(2):353-74. doi: 10.1016/s0193-953x(05)70317-8
[10]Dienemann J, Boyle E, Baker D, Resnick W, Wiederhorn N, Campbell J. Intimate partner abuse among women diagnosed with depression. Issues in Mental Health Nursing. 2000; 21(5):499-513. doi: 10.1080/01612840050044258
[11]Jones L, Hughes M, Unterstaller U. Post-Traumatic Stress Disorder (PTSD) in victims of domestic violence: A review of the research. Trauma, Violence, & Abuse. 2001; 2(2):99-119. doi: 10.1177/1524838001002002001
[12]Stein MB, Kennedy C. Major depressive and post-traumatic stress disorder comorbidity in female victims of intimate partner violence. Journal of Affective Disorders. 2001; 66(2-3):133-8. doi: 10.1016/s0165-0327(00)00301-3
[13]Straus MA, Gelles RJ, Smith C. Physical violence in American families: Risk factors and adaptations to violence in 8,145 families. New Brunswick, NJ: Transaction Publishers; 1990.
[14]Hilberman E, Munson K. Sixty battered women. Victimology. 1977; 2(3-4): 460-470.
[15]Bonomi AE, Anderson ML, Reid RJ, Rivara FP, Carrell D, Thompson RS. Medical and psychosocial diagnoses in women with a history of intimate partner violence. Archives of Internal Medicine. 2009; 169(18):1692-7. doi: 10.1001/archinternmed.2009.292
[16]Tsai AC, Tomlinson M, Comulada WS, Rotheram-Borus MJ. Intimate partner violence and depression symptom severity among South African women during pregnancy and postpartum: Population-based prospective cohort study. PLOS Medicine. 2016; 13(1):1001943. doi: 10.1371/journal.pmed.1001943
[17]Golding JM. Intimate partner violence as a risk factor for mental disorders: A meta-analysis. Journal of Family Violence. 1999; 14(2):99-132. doi: 10.1023/A:1022079418229
[18]Mapayi B, Makanjuola RO, Mosaku SK, Adewuya OA, Afolabi O, Aloba OO, et al. Impact of intimate partner violence on anxiety and depression amongst women in Ile-Ife, Nigeria. Archives of Women's Mental Health. 2013; 16(1):11-8. doi: 10.1007/s00737-012-0307-x
[19]Wong J, Mellor D. Intimate partner violence and women’s health and wellbeing: Impacts, risk factors and responses. Contemporary Nurse. 2014; 46(2):170-9. doi: 10.5172/conu.2014.46.2.170
[20]Estefan LF, Coulter ML, VandeWeerd C. Depression in women who have left violent relationships: The unique impact of frequent emotional abuse. Violence Against Women. 2016; 12(11): 1397 to 1413. doi: 10.1177/1077801215624792
[21]Davins-Pujols M, Pérez-Testor C, Salamero-Baró M, Castillo-Garayoa JA. Personality profiles in abused women receiving psychotherapy according to the existence of childhood abuse. Journal of Family Violence. 2012; 27(2):87-96. doi: 10.1007/s10896-011-9407-z
[22]Torres A, Garcia-Esteve L, Navarro P, Tarragona MJ, Imaz ML, Ascaso C, et al. Relationship between intimate partner violence, depressive symptomatology, and personality traits. Journal of Family Violence. 2013; 28(4):369-79. doi: 10.1007/s10896-013-9502-4
[23]Gellen MI, Hoffman RA, Jones M, Stone M. Abused and nonabused women: MMPI profile differences. The Personnel and Guidance Journal. 1984; 62(10):601-4. doi: 10.1111/j.2164-4918.1984.tb00134.x
[24]Jang KL, Stein MB, Taylor S, Asmundson GJ, Livesley WJ. Exposure to traumatic events and experiences: aetiological relationships with personality function. Psychiatry Research. 2003; 120(1):61-9. doi: 10.1016/s0165-1781(03)00172-0
[25]Löckenhoff CE, Terracciano A, Patriciu NS, Eaton WW, Costa PT. Self‐reported extremely adverse life events and longitudinal changes in five‐factor model personality traits in an urban sample. Journal of Traumatic Stress. 2009; 22(1):53-9. doi: 10.1002/jts.20385
[26]Motevaliyan SM, Yaacob SN, Juhari R, Mansor M, Dokoushkani F, Watson PJ. Associations of personality traits and childhood insult experience with perceived husbands’ psychological aggression among Iranian women. Journal of Family Violence. 2016. doi: 10.1007/s10896-016-9811-5
[27]Estrellado AF. Assessing the personality profile of battered women. In: Faulkner AG, editor. The Assessment Handbook. Coleraine: Ulster University; 2010.
[28]Yaghubkhani Ghiasvand M, Fathi Aghdam G. [Personality correlates of emotionally abused students with opposite sex (Persian)]. Journal of Qazvin University of Medical Sciences. 2012; 16(3):61-65.
[29]Panaghi L, Pirouzi D, Shirinbayan M, Ahmadi Z. [The role of personality and demographic traits in spouse abuse (Persian)].Iranian Journal of Psychiatry and Clinical Psychology. 2011; 17(2):126-135.
[30]Ghahari SH, Atefvahid MK, Yousefi H. [The prevalence of spouse abuse among married students of Islamic Azad University of Tonekabon in 2004 (Persian)]. Journal of Mazandaran University of Medical Sciences. 2006; 15(50):83-89.
[31]Dasarband B. [The moderating role of personality characteristics and stress coping strategies in the relation between spouse abuse with women’s depressive symptoms and couple burnout (Persian)] [MA thesis]. Tehran: Shahid Beheshti University; 2015.
[32]Stefan-Dabson K, Mohammadkhani P, Massah-Choulabi O. [Psychometrics characteristic of Beck depression Inventory-II in patients with major depressive disorder (Persian)]. Journal of Rehabilitation. 2007; 8:80-86.
[33]Fata L, Birshak B, Atefvahid MK, Dabson KS. [Meaning assignment structure/ schema, emotional states and cognitive processing of emotional information: Comparing two conceptual frameworks (Persian)]. Iranian Journal of Psychiatry and Clinical Psychology. 2005; 11(3):312-326.
[34]Roshan Chosli R, Shaeiri M, Atri Fard M, Nikkhah A, Ghaem Maghami B, Rahimi Rad A. [Investigating psychometric properties of “NEO-Five Factor Inventory” (NEO-FFI) (Persian)]. Daneshvar Raftar. 2006; 13(16):27-36.
[35]Aliloo MM, Arji A, Bakhshipoor Rudsari A, Shahjui T. [The relation between personality and coping strategies in drug users with HIV (Persian)]. Medical Journal of Tabriz University of Medical Sciences & Health Services. 2009; 1(33):70-76.
[36]Barnett OW. Why battered women do not leave, Part 2 external inhibiting factors—social support and internal inhibiting factors. Trauma, Violence, & Abuse. 2001; 2(1):3-35. doi: 10.1177/1524838001002001001
[37]Walker LE. Psychology and domestic violence around the world. American Psychologist. 1999; 54(1):21-29. doi: 10.1037//0003-066x.54.1.21
[38]Miller JB. The development of women’s sense of self. In: Jordan JV, Kaplan AG, Stiver IP, Surrey JL, Baker Miller J, editors. Women’s Growth in Connection: Writings from the Stone Center. New York: Guilford Press; 1991.
[39]Craven Z. Battered woman syndrome. Australian Domestic & Family Violence Clearinghouse; Philadelphia: Sage; 2003.
[40]Finch JF, Graziano WG. Predicting depression from temperament, personality, and patterns of social relations. Journal of Personality. 2001; 69(1):27-55. doi: 10.1111/1467-6494.00135
[41]van Straten A, Cuijpers P, van Zuuren FJ, Smits N, Donker M. Personality traits and health-related quality of life in patients with mood and anxiety disorders. Quality of Life Research. 2006; 16(1):1-8. doi: 10.1007/s11136-006-9124-x
[42]Costa PT, McCrae RR. Neo PI/FFI manual supplement. Odessa, FL: Psychological Assessment Resources. 1989.
[43]Graziano WG, Jensen-Campbell LA, Hair EC. Perceiving interpersonal conflict and reacting to it: the case for agreeableness. Journal of Personality and Social Psychology. 1996; 70(4):820-835. doi: 10.1037//0022-3514.70.4.820
Full-Text: (6647 Views)
Extended Abstract
1. Introduction
Violence against women is one of the most important human rights and health problems across the world [1, 2]. It affects the rights, health, well-being, and personality of women and poses a serious threat to the family and society [3]. The most common form of violence against women is domestic violence, i.e., violent abuse by the spouse .
Violence against a spouse is associated with physical injuries [8], poor mental health [9] including depression, anxiety, post-traumatic stress disorder, and suicidal thoughts and actions [10-12]. In such cases, depression disorders and suicide attempts in women victims of violence is four times higher than that in non-victimized women [13].
Given this background , can we say that women victims of violence experience more symptoms of depression than other women? If this is the case, what can change the likelihood of these outcomes in women victims. In an attempt to answer these research questions , the present study investigates the moderating role of personality traits in relation to domestic violence and depression.
2. Method
This correlational study is descriptive in form. The study population consisted of all married women in Tehran in 1393 (2014). Sample size was determined to be 302 subjects based on the number of predictor variables. To select the appropriate sample, convenient sampling method was employed, and 400 questionnaires were distributed in different places of the city including parks, shopping centers and cultural centers in five regions (North, South, East, West and Central). After obtaining informed consent to participate in the study, the participants were asked to respond to the questionnaire. The researcher monitored the overall process while the participants were answering the questions . Inclusion criteria for women participating in the study are living in Tehran and being married and having permanent first and second marriage . Exclusion criteria included a history of psychiatric disease and divorce or the separation of the couple. Of the 400 questionnaires obtained, 98 incomplete questionnaires were excluded.
After converting the scores into standard scores, hierarchical regression was used for five personality traits and three types of violence against women so as to investigate the moderating role of personality traits of women in the relationship between domestic violence and depression. The personality scores considered in this study were neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness, and the three types of violence against women included psychological violence, physical violence, and sexual violence. The dependent variable was scores of depression symptoms. Data analysis was performed with the help of SPSS-22 software using the hierarchical regression analysis.
3. Results
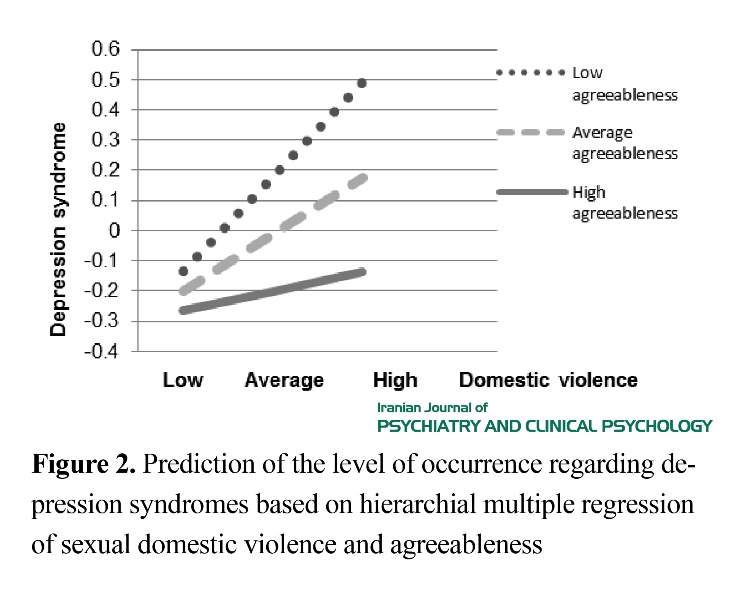
A total of 302 patients participated in the study. The average age and duration of marriage for women in the research were found to be 38.59 years and 16.10 years, respectively. The mean and standard deviation of research variables for women participating in the study can be seen in Table 1. Based on the Figures 1 and 2, it can be inferred that those who are agreeable to a greater extent showed fewer symptoms of depression compared with people who have relatively average or lesser extent of this trait. But when sexual violence was low, the difference between the three groups was negligible. The more the sexual violence, the greater was the difference between the three groups of violence . Regarding the difference in the slope of the three figures, it should be noted that the more the agreeable a person is, the greater the sexual abuse of the spouse can predict the symptoms of depression (Figure 2).
4. Discussion and Conclusion
Our findings support the direct connection between domestic violence against women and their depression symptoms. In other words, women who are exposed to domestic violence experience significant depressive symptoms. Previous research also suggests that women who are subjected to violence by their husbands are more depressed than other women [16, 19, 31].
This finding can be explained using the theory of “battered women syndrome” proposed by Walker [37], which is based on Seligman's theory of learned helplessness.
1. Introduction
Violence against women is one of the most important human rights and health problems across the world [1, 2]. It affects the rights, health, well-being, and personality of women and poses a serious threat to the family and society [3]. The most common form of violence against women is domestic violence, i.e., violent abuse by the spouse .
Violence against a spouse is associated with physical injuries [8], poor mental health [9] including depression, anxiety, post-traumatic stress disorder, and suicidal thoughts and actions [10-12]. In such cases, depression disorders and suicide attempts in women victims of violence is four times higher than that in non-victimized women [13].
Given this background , can we say that women victims of violence experience more symptoms of depression than other women? If this is the case, what can change the likelihood of these outcomes in women victims. In an attempt to answer these research questions , the present study investigates the moderating role of personality traits in relation to domestic violence and depression.
2. Method
This correlational study is descriptive in form. The study population consisted of all married women in Tehran in 1393 (2014). Sample size was determined to be 302 subjects based on the number of predictor variables. To select the appropriate sample, convenient sampling method was employed, and 400 questionnaires were distributed in different places of the city including parks, shopping centers and cultural centers in five regions (North, South, East, West and Central). After obtaining informed consent to participate in the study, the participants were asked to respond to the questionnaire. The researcher monitored the overall process while the participants were answering the questions . Inclusion criteria for women participating in the study are living in Tehran and being married and having permanent first and second marriage . Exclusion criteria included a history of psychiatric disease and divorce or the separation of the couple. Of the 400 questionnaires obtained, 98 incomplete questionnaires were excluded.
After converting the scores into standard scores, hierarchical regression was used for five personality traits and three types of violence against women so as to investigate the moderating role of personality traits of women in the relationship between domestic violence and depression. The personality scores considered in this study were neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness, and the three types of violence against women included psychological violence, physical violence, and sexual violence. The dependent variable was scores of depression symptoms. Data analysis was performed with the help of SPSS-22 software using the hierarchical regression analysis.
3. Results
A total of 302 patients participated in the study. The average age and duration of marriage for women in the research were found to be 38.59 years and 16.10 years, respectively. The mean and standard deviation of research variables for women participating in the study can be seen in Table 1. Based on the Figures 1 and 2, it can be inferred that those who are agreeable to a greater extent showed fewer symptoms of depression compared with people who have relatively average or lesser extent of this trait. But when sexual violence was low, the difference between the three groups was negligible. The more the sexual violence, the greater was the difference between the three groups of violence . Regarding the difference in the slope of the three figures, it should be noted that the more the agreeable a person is, the greater the sexual abuse of the spouse can predict the symptoms of depression (Figure 2).
4. Discussion and Conclusion
Our findings support the direct connection between domestic violence against women and their depression symptoms. In other words, women who are exposed to domestic violence experience significant depressive symptoms. Previous research also suggests that women who are subjected to violence by their husbands are more depressed than other women [16, 19, 31].
This finding can be explained using the theory of “battered women syndrome” proposed by Walker [37], which is based on Seligman's theory of learned helplessness.


Walker defined the “battered women syndrome” using diagnostic terms such as "growth of symptoms and physical, psychological and social abnormalities such as depression, low self-esteem, and isolation, which occur as a result of experiencing violence from the husband" [37]. According to Walker, with passing time and with repeated uncontrollable and unpredictable courses of violence, abused women realize that their actions made no change in the relationship [38], and they lose a sense of control over the stressful situations. As a result, they feel helpless to stop the violence, which in turn causes their depression [39].
According to our study results, those who are agreeable to a greater extent manifested fewer depressive symptoms compared to people who have medium and low levels of this trait. When the psychological violence was low, the difference between the three groups was negligible. When the psychological and sexual violence increased, the difference between the three groups also increased. In other words, the lesser the women are agreeable, the more the psychological violence inflicting upon them can determine the levels of depressive symptoms.
According to the research by Schutte et al. (2014 ), personality trait of agreeableness has a significant negative relationship with self-criticism and depression scores. In this regard, Finch and Graziano [40] showed that personality trait of agreeableness is indirectly associated with depression. Agreeable people have more friends, receive more social support, and apply effective reactions, which makes them less likely to have depression [41].
To explain this finding, we can use the traits of agreeableness structures. People who have more of this trait are considered to be trustworthy, optimist, and cooperative in interpersonal relationships. They are polite, warm, loving, flexible, generous, gentle, caring, thoughtful, and logical persons. Such people desire to help other people and look at them in a positive way [42]. In addition, agreeable people interpret social behaviors of others as less aggressive, and they tend to be more involved in social relations that facilitate comm::::::::::union:::::::::: [43]. These traits and having a positive attitude towards the people and events will cause agreeable women victims of domestic violence to be less depressed compared with others.
The current study showed that women who are inflicted with domestic violence are significantly more prone to depression and that victims who are agreeable have fewer depressive symptoms. In this study, we investigated the role of individual variables in violent relationships of married couples while one of the main variables in the field is the relationship between married couples.
Acknowledgments
Deputy of Research and Family Research Center, Faculty of Education and Psychology, Shahid Beheshti University, Tehran, Iran, have financially supported the present paper.
Conflict of Interest
The authors declared no conflicts of interest.
According to our study results, those who are agreeable to a greater extent manifested fewer depressive symptoms compared to people who have medium and low levels of this trait. When the psychological violence was low, the difference between the three groups was negligible. When the psychological and sexual violence increased, the difference between the three groups also increased. In other words, the lesser the women are agreeable, the more the psychological violence inflicting upon them can determine the levels of depressive symptoms.
According to the research by Schutte et al. (2014 ), personality trait of agreeableness has a significant negative relationship with self-criticism and depression scores. In this regard, Finch and Graziano [40] showed that personality trait of agreeableness is indirectly associated with depression. Agreeable people have more friends, receive more social support, and apply effective reactions, which makes them less likely to have depression [41].
To explain this finding, we can use the traits of agreeableness structures. People who have more of this trait are considered to be trustworthy, optimist, and cooperative in interpersonal relationships. They are polite, warm, loving, flexible, generous, gentle, caring, thoughtful, and logical persons. Such people desire to help other people and look at them in a positive way [42]. In addition, agreeable people interpret social behaviors of others as less aggressive, and they tend to be more involved in social relations that facilitate comm::::::::::union:::::::::: [43]. These traits and having a positive attitude towards the people and events will cause agreeable women victims of domestic violence to be less depressed compared with others.
The current study showed that women who are inflicted with domestic violence are significantly more prone to depression and that victims who are agreeable have fewer depressive symptoms. In this study, we investigated the role of individual variables in violent relationships of married couples while one of the main variables in the field is the relationship between married couples.
Acknowledgments
Deputy of Research and Family Research Center, Faculty of Education and Psychology, Shahid Beheshti University, Tehran, Iran, have financially supported the present paper.
Conflict of Interest
The authors declared no conflicts of interest.
مقدمه
خشونت علیه زنان، یکی از مهمترین مشکلات حقوق بشر و سلامتی در سطح جهان به شمار میرود [2 ،1] که نه تنها حقوق، سلامت، رفاه و شخصیت زنان، بلکه بنیان خانواده و جامعه را نیز با تهدید جدی مواجه میکند [3]. شایعترین خشونت علیه زنان، توسط همسر صورت میگیرد و با عنوان همسرآزاری علیه زنان شناخته میشود [4] که عبارت است از اعمال هرگونه بدرفتاری عمدی نسبت به زن توسط همسر [5]. آمار سازمان جهانی بهداشت بیانگر آن است که شریک زندگی 16 تا 52 درصد زنان با آنان با خشونت رفتار میکنند [6]. در پیمایش ملی گستردهای که در 28 استان ایران در سال 1388 صورت گرفت، گزارشها نشان داد که 66 درصد زنان حداقل یک بار در طول زندگی مشترک خود با خشونت همسر مواجه میشوند [7].
خشونت علیه همسر با صدمات جسمی [8]، سلامت روان ضعیف [9] شامل افسردگی، اضطراب، اختلال استرس پس از سانحه و افکار و اقدامات خودکشی مرتبط است [12-10]. افسردگی و اقدام به خودکشی در زنان قربانی خشونت چهار برابر بیشتر از زنان غیرقربانی دیده میشود [13].
افسردگی اصلیترین پیامد روانشناختی همسرآزاری است [16-14 ،12] که به گزارش گولدینگ [17] میانگین آن در زنان قربانی همسرآزاری، 6/47 درصد است. احتمال افسردگی در زنان خشونتدیده، ده برابر زنان غیرقربانی است [20-18].
حال با توجه به پیامدهای مشکلآفرین خشونت، موضوع مهم دیگر در این زمینه بررسی عواملی است که احتمال وقوع پیامدهایی همچون افسردگی را در زنان قربانی تغییر میدهند.
بسیاری از محققان معتقدند که همسرآزاری علیه زنان، میتواند بر تمامی سطوح عملکرد آنها تأثیر بگذارد و حتی سبک شخصیتی زنان قربانی را نیز تغییر دهد [21]. مطالعات انجامشده در حوزه ویژگیهای شخصیتی زنان قربانی همسرآزاری، نتایج متناقضی را دربرداشته است؛ از این رو تفسیر ارتباط میان این دو متغیر نیز موضوعی بحثانگیز است [22]. از یکسو مطالعات اولیه در این حوزه، بر ویژگیهای شخصیتی زنان قربانی تمرکز کردند و نشان دادند که آسیبهای شخصیتی، احتمال خشونت دیدن زنان را افزایش میدهد [23] و زنان با ویژگیهای شخصیتی خاصی، آمادگی قرارگرفتن در معرض همسرآزاری را بیشتر دارند [24]؛ از سویی دیگر، برخی پژوهشگران به این نتیجه دست یافتند که همسرآزاری میتواند بر شخصیت زنان قربانی تأثیر بگذارد [23] و منجر به الگویی از تغییرات در صفات شخصیتی فرد از جمله افزایش روانرنجورخویی و کاهش توافقجویی شود [26 ،25].
در مطالعاتی که با پرسشنامه شخصیتی چند محوری بالینی میلون انجام شد، نمرات مقیاسهای اسکیزوئید، اجتناب و خودسرکوبگری در زنان قربانی خشونت بالا بود [27]. یعقوب خانی غیاثوند و فتحی اقدم [28] در پژوهش خود از پرسشنامه شخصیتی نئو استفاده کردند و نشان دادند به زنان برونگراتر، بیشتر خشونت میشود. همچنین آنها در مطالعه خود به این نتیجه دست یافتند که به افراد توافقپذیرتر، کمتر خشونت میشود. در همین راستا، پناغی، پیروزی، شیرینبیان و احمدی [29] گزارش کردند که روانآزردهخویی بیشترین همبستگی را با خشونتدیدگی دارد. وظیفهشناسی در پیشبینی خشونت جنسی و برونگرایی در پیشبینی خشونت جسمانی سهم منفی دارد.
اکنون با توجه به اهمیت همسرآزاری علیه زنان و پیامدهای مشکلآفرین آن از جمله افسردگی، آیا میتوان گفت که زنان قربانی خشونت در مقایسه با زنان دیگر علائم افسردگی بیشتری دارند؟ اگر اینگونه است، چه عواملی احتمال وقوع این پیامدها را در زنان قربانی تغییر میدهد؟ در همین راستا در پژوهش حاضر به بررسی نقش تعدیلکنندگی ویژگیهای شخصیتی در رابطه همسرآزاری و نشانگان افسردگی پرداخته شده است.
روش
جامعه آماری و نمونه مورد مطالعه و روش نمونهگیری
روش پژوهش حاضر، توصیفی از نوع همبستگی است. جامعه آماری شامل تمامی زنان متأهل ساکن شهر تهران در سال 1393 است. حجم نمونه بر اساس تعداد متغیرهای پیش بین 302 نفر تعیین شد. برای انتخاب نمونه مناسبتر، 400 پرسشنامه در مکانهای مختلف شهر ازجمله پارکها، مراکز خرید، فرهنگسراها در پنج منطقه تهران (شمال، جنوب، شرق، غرب و مرکز) به روش نمونهگیری در دسترس توزیع شد، به این ترتیب که شرکتکنندگان پس از اعلام رضایت برای شرکت در پژوهش، به سؤالات پرسشنامهها پاسخ دادند. از فرد پرسیده میشد که آیا سابقه مراجعه به روانپزشک و مصرف دارو داشته یا نه. پژوهشگر در حین پاسخدهی شرکتکنندگان، بر روند تکمیل پرسشنامهها نظارت داشت و به سؤالات احتمالی آنها پاسخ میداد. در آخر 98 پرسشنامه ناقص حذف شدند. ملاکهای ورود زنان شرکتکننده در این پژوهش عبارت است از: ساکن شهر تهران و متأهل بودن، ازدواج اول و ازدواج دائم داشتن. معیارهای خروج نیز شامل سابقه بیماری روانپزشکی و متقاضی طلاق یا در متارکه بودن زن و شوهر است.
ابزار
پرسشنامه همسرآزاری
قهاری، عاطف وحید و یوسفی در سال 1384 پرسشنامه همسرآزاری را تدوین کردهاند [30]. در پژوهش حاضر، از این پرسشنامه برای ارزیابی همسرآزاری علیه زنان استفاده شده است. این پرسشنامه دارای 44 ماده است که 20 ماده آن خشونت عاطفی، 10 ماده خشونت جسمانی و 14 ماده خشونت جنسی را میسنجند. هر بخش این پرسشنامه دارای چهار گزینه هرگز، گاهی، اغلب و همیشه است. شیوه نمرهگذاری این پرسشنامه بدینصورت است که گزینه هرگز نمره صفر، گاهی نمره 1، اغلب نمره 2 و گزینه همیشه نمره 3 میگیرد. بدین ترتیب حداکثر نمره 132 و حداقل آن صفر است.
استادان روانپزشکی و روانشناسی بالینی انستیتو روانپزشکی تهران روایی صوری و محتوایی پرسشنامه را تأیید کردهاند و برای تعیین پایایی درونی آن از ضریب آلفای کرونباخ استفاده شده است. نتایج نشان داده که ضریب آلفای کرونباخ 92/0 است [29]. پایایی این پرسشنامه از طریق روش آزمونآزمون مجدد برای خشونت روانی 95/0، خشونت جسمانی 87/0 و برای خشونت جنسی 87/0 گزارش شد [31].
پرسشنامه افسردگی بک (شکل بازنگریشده)
آرون تی. بک در سال 1961 پرسشنامه افسردگی بک را تدوین کرد و در سال 1996 بک، استیر و براون شکل بازنگریشده آن را منتشر کردند. این پرسشنامه برای سنجش شدت افسردگی در افرادی به کار میرود که تشخیص افسردگی دریافت کردهاند [37].
در پژوهش حاضر از شکل بازنگریشده آن برای ارزیابی نشانههای افسردگی در زنان استفاده شده است. این پرسشنامه، یک مقیاس خودگزارشدهی 21 سؤالی است که هر سؤال آن دارای چهار گزینه با نمره صفر تا سه است. حداکثر نمره 63 و حداقل آن صفر است.
ضریب همسانی درونی این پرسشنامه در جامعه بهنجار 81/0 گزارش شده است. ضریب اعتبار کل برای هر 21 سؤال 913/0 به دست آمد [32]. ضریب همبستگی میان دو نیمه 89/0 و ضریب بازآزمایی با فاصله یک هفته 94/0بود [33].
پرسشنامه شخصیت 5 عاملی نئو (نسخه تجدیدنظرشده)
کاستا و مک کری در سال 1985پرسشنامه شخصیت نئو را طراحی کردند که نسخه کوتاه آن شامل 60 ماده است [34]. در پژوهش حاضر نیز از همین فرم برای ارزیابی ویژگیهای شخصیتی زنان استفاده میشود.
این پرسشنامه پنج عامل را در شخصیت افراد بررسی میکند که عبارتند از: روانآزردهخویی، برونگرایی، گشودگی به تجربه، توافقی بودنو مسئولیتپذیری. هر یک از ویژگیهای مذکور با 12 سؤال اندازهگیری میشوند و نمرهای از صفر تا 48 دارند [35].
کاستا و مککری (1992) ضریب آلفای 68/0 (برای توافق جویی) و 86/0 (برای روان آزرده خویی) را گزارش کردهاند. این ابزار 85 درصد واریانس را در اعتبار همگرا تبیین میکند. آنها در یک مطالعه ، ضریب پایایی بین 82/0 تا 51/0 برای 18 صفت فرعی N,E,O و 81/0 تا 63/0 برای عوامل اصلی پنجگانه در مردان و زنان به دست آوردند.
در ایران در مطالعهای روشن، چسلی و همکاران [39] ضرایب آلفای کرونباخ به ترتیب حداکثر و حداقل را برای روان رنجوری 83/0 وگشودگی 35/0به دست آوردند. در این مطالعه اعتبار آزمون مجدد در فاصله یک هفته برای برونگرایی 82/0 و برای گشودگی به تجربه 61/0 محاسبه شد. تجزیهوتحلیل دادهها با کمک نرمافزار SPSS22 و به روش رگرسیون سلسله مراتبی انجام شد.
یافتهها
در مجموع 302 نفر در پژوهش شرکت کردند. میانگین سن و مدت ازدواج زنان شرکتکننده در پژوهش به ترتیب 59/38 و 10/16 است. میانگین و انحراف استاندارد مربوط به متغیرهای پژوهش در زنان شرکت کننده در جدول شماره 1 مشاهده میشود.
برای بررسی نقش تعدیلکنندگی ویژگیهای شخصیتی زنان در رابطه بین همسرآزاری و افسردگی، بعد از تبدیل نمرات به نمرات استاندارد، از روش رگرسیون سلسله مراتبی بین پنج ویژگی شخصیتی (روانرنجورخویی، برونگرایی، گشودگی به
خشونت علیه زنان، یکی از مهمترین مشکلات حقوق بشر و سلامتی در سطح جهان به شمار میرود [2 ،1] که نه تنها حقوق، سلامت، رفاه و شخصیت زنان، بلکه بنیان خانواده و جامعه را نیز با تهدید جدی مواجه میکند [3]. شایعترین خشونت علیه زنان، توسط همسر صورت میگیرد و با عنوان همسرآزاری علیه زنان شناخته میشود [4] که عبارت است از اعمال هرگونه بدرفتاری عمدی نسبت به زن توسط همسر [5]. آمار سازمان جهانی بهداشت بیانگر آن است که شریک زندگی 16 تا 52 درصد زنان با آنان با خشونت رفتار میکنند [6]. در پیمایش ملی گستردهای که در 28 استان ایران در سال 1388 صورت گرفت، گزارشها نشان داد که 66 درصد زنان حداقل یک بار در طول زندگی مشترک خود با خشونت همسر مواجه میشوند [7].
خشونت علیه همسر با صدمات جسمی [8]، سلامت روان ضعیف [9] شامل افسردگی، اضطراب، اختلال استرس پس از سانحه و افکار و اقدامات خودکشی مرتبط است [12-10]. افسردگی و اقدام به خودکشی در زنان قربانی خشونت چهار برابر بیشتر از زنان غیرقربانی دیده میشود [13].
افسردگی اصلیترین پیامد روانشناختی همسرآزاری است [16-14 ،12] که به گزارش گولدینگ [17] میانگین آن در زنان قربانی همسرآزاری، 6/47 درصد است. احتمال افسردگی در زنان خشونتدیده، ده برابر زنان غیرقربانی است [20-18].
حال با توجه به پیامدهای مشکلآفرین خشونت، موضوع مهم دیگر در این زمینه بررسی عواملی است که احتمال وقوع پیامدهایی همچون افسردگی را در زنان قربانی تغییر میدهند.
بسیاری از محققان معتقدند که همسرآزاری علیه زنان، میتواند بر تمامی سطوح عملکرد آنها تأثیر بگذارد و حتی سبک شخصیتی زنان قربانی را نیز تغییر دهد [21]. مطالعات انجامشده در حوزه ویژگیهای شخصیتی زنان قربانی همسرآزاری، نتایج متناقضی را دربرداشته است؛ از این رو تفسیر ارتباط میان این دو متغیر نیز موضوعی بحثانگیز است [22]. از یکسو مطالعات اولیه در این حوزه، بر ویژگیهای شخصیتی زنان قربانی تمرکز کردند و نشان دادند که آسیبهای شخصیتی، احتمال خشونت دیدن زنان را افزایش میدهد [23] و زنان با ویژگیهای شخصیتی خاصی، آمادگی قرارگرفتن در معرض همسرآزاری را بیشتر دارند [24]؛ از سویی دیگر، برخی پژوهشگران به این نتیجه دست یافتند که همسرآزاری میتواند بر شخصیت زنان قربانی تأثیر بگذارد [23] و منجر به الگویی از تغییرات در صفات شخصیتی فرد از جمله افزایش روانرنجورخویی و کاهش توافقجویی شود [26 ،25].
در مطالعاتی که با پرسشنامه شخصیتی چند محوری بالینی میلون انجام شد، نمرات مقیاسهای اسکیزوئید، اجتناب و خودسرکوبگری در زنان قربانی خشونت بالا بود [27]. یعقوب خانی غیاثوند و فتحی اقدم [28] در پژوهش خود از پرسشنامه شخصیتی نئو استفاده کردند و نشان دادند به زنان برونگراتر، بیشتر خشونت میشود. همچنین آنها در مطالعه خود به این نتیجه دست یافتند که به افراد توافقپذیرتر، کمتر خشونت میشود. در همین راستا، پناغی، پیروزی، شیرینبیان و احمدی [29] گزارش کردند که روانآزردهخویی بیشترین همبستگی را با خشونتدیدگی دارد. وظیفهشناسی در پیشبینی خشونت جنسی و برونگرایی در پیشبینی خشونت جسمانی سهم منفی دارد.
اکنون با توجه به اهمیت همسرآزاری علیه زنان و پیامدهای مشکلآفرین آن از جمله افسردگی، آیا میتوان گفت که زنان قربانی خشونت در مقایسه با زنان دیگر علائم افسردگی بیشتری دارند؟ اگر اینگونه است، چه عواملی احتمال وقوع این پیامدها را در زنان قربانی تغییر میدهد؟ در همین راستا در پژوهش حاضر به بررسی نقش تعدیلکنندگی ویژگیهای شخصیتی در رابطه همسرآزاری و نشانگان افسردگی پرداخته شده است.
روش
جامعه آماری و نمونه مورد مطالعه و روش نمونهگیری
روش پژوهش حاضر، توصیفی از نوع همبستگی است. جامعه آماری شامل تمامی زنان متأهل ساکن شهر تهران در سال 1393 است. حجم نمونه بر اساس تعداد متغیرهای پیش بین 302 نفر تعیین شد. برای انتخاب نمونه مناسبتر، 400 پرسشنامه در مکانهای مختلف شهر ازجمله پارکها، مراکز خرید، فرهنگسراها در پنج منطقه تهران (شمال، جنوب، شرق، غرب و مرکز) به روش نمونهگیری در دسترس توزیع شد، به این ترتیب که شرکتکنندگان پس از اعلام رضایت برای شرکت در پژوهش، به سؤالات پرسشنامهها پاسخ دادند. از فرد پرسیده میشد که آیا سابقه مراجعه به روانپزشک و مصرف دارو داشته یا نه. پژوهشگر در حین پاسخدهی شرکتکنندگان، بر روند تکمیل پرسشنامهها نظارت داشت و به سؤالات احتمالی آنها پاسخ میداد. در آخر 98 پرسشنامه ناقص حذف شدند. ملاکهای ورود زنان شرکتکننده در این پژوهش عبارت است از: ساکن شهر تهران و متأهل بودن، ازدواج اول و ازدواج دائم داشتن. معیارهای خروج نیز شامل سابقه بیماری روانپزشکی و متقاضی طلاق یا در متارکه بودن زن و شوهر است.
ابزار
پرسشنامه همسرآزاری
قهاری، عاطف وحید و یوسفی در سال 1384 پرسشنامه همسرآزاری را تدوین کردهاند [30]. در پژوهش حاضر، از این پرسشنامه برای ارزیابی همسرآزاری علیه زنان استفاده شده است. این پرسشنامه دارای 44 ماده است که 20 ماده آن خشونت عاطفی، 10 ماده خشونت جسمانی و 14 ماده خشونت جنسی را میسنجند. هر بخش این پرسشنامه دارای چهار گزینه هرگز، گاهی، اغلب و همیشه است. شیوه نمرهگذاری این پرسشنامه بدینصورت است که گزینه هرگز نمره صفر، گاهی نمره 1، اغلب نمره 2 و گزینه همیشه نمره 3 میگیرد. بدین ترتیب حداکثر نمره 132 و حداقل آن صفر است.
استادان روانپزشکی و روانشناسی بالینی انستیتو روانپزشکی تهران روایی صوری و محتوایی پرسشنامه را تأیید کردهاند و برای تعیین پایایی درونی آن از ضریب آلفای کرونباخ استفاده شده است. نتایج نشان داده که ضریب آلفای کرونباخ 92/0 است [29]. پایایی این پرسشنامه از طریق روش آزمونآزمون مجدد برای خشونت روانی 95/0، خشونت جسمانی 87/0 و برای خشونت جنسی 87/0 گزارش شد [31].
پرسشنامه افسردگی بک (شکل بازنگریشده)
آرون تی. بک در سال 1961 پرسشنامه افسردگی بک را تدوین کرد و در سال 1996 بک، استیر و براون شکل بازنگریشده آن را منتشر کردند. این پرسشنامه برای سنجش شدت افسردگی در افرادی به کار میرود که تشخیص افسردگی دریافت کردهاند [37].
در پژوهش حاضر از شکل بازنگریشده آن برای ارزیابی نشانههای افسردگی در زنان استفاده شده است. این پرسشنامه، یک مقیاس خودگزارشدهی 21 سؤالی است که هر سؤال آن دارای چهار گزینه با نمره صفر تا سه است. حداکثر نمره 63 و حداقل آن صفر است.
ضریب همسانی درونی این پرسشنامه در جامعه بهنجار 81/0 گزارش شده است. ضریب اعتبار کل برای هر 21 سؤال 913/0 به دست آمد [32]. ضریب همبستگی میان دو نیمه 89/0 و ضریب بازآزمایی با فاصله یک هفته 94/0بود [33].
پرسشنامه شخصیت 5 عاملی نئو (نسخه تجدیدنظرشده)
کاستا و مک کری در سال 1985پرسشنامه شخصیت نئو را طراحی کردند که نسخه کوتاه آن شامل 60 ماده است [34]. در پژوهش حاضر نیز از همین فرم برای ارزیابی ویژگیهای شخصیتی زنان استفاده میشود.
این پرسشنامه پنج عامل را در شخصیت افراد بررسی میکند که عبارتند از: روانآزردهخویی، برونگرایی، گشودگی به تجربه، توافقی بودنو مسئولیتپذیری. هر یک از ویژگیهای مذکور با 12 سؤال اندازهگیری میشوند و نمرهای از صفر تا 48 دارند [35].
کاستا و مککری (1992) ضریب آلفای 68/0 (برای توافق جویی) و 86/0 (برای روان آزرده خویی) را گزارش کردهاند. این ابزار 85 درصد واریانس را در اعتبار همگرا تبیین میکند. آنها در یک مطالعه ، ضریب پایایی بین 82/0 تا 51/0 برای 18 صفت فرعی N,E,O و 81/0 تا 63/0 برای عوامل اصلی پنجگانه در مردان و زنان به دست آوردند.
در ایران در مطالعهای روشن، چسلی و همکاران [39] ضرایب آلفای کرونباخ به ترتیب حداکثر و حداقل را برای روان رنجوری 83/0 وگشودگی 35/0به دست آوردند. در این مطالعه اعتبار آزمون مجدد در فاصله یک هفته برای برونگرایی 82/0 و برای گشودگی به تجربه 61/0 محاسبه شد. تجزیهوتحلیل دادهها با کمک نرمافزار SPSS22 و به روش رگرسیون سلسله مراتبی انجام شد.
یافتهها
در مجموع 302 نفر در پژوهش شرکت کردند. میانگین سن و مدت ازدواج زنان شرکتکننده در پژوهش به ترتیب 59/38 و 10/16 است. میانگین و انحراف استاندارد مربوط به متغیرهای پژوهش در زنان شرکت کننده در جدول شماره 1 مشاهده میشود.
برای بررسی نقش تعدیلکنندگی ویژگیهای شخصیتی زنان در رابطه بین همسرآزاری و افسردگی، بعد از تبدیل نمرات به نمرات استاندارد، از روش رگرسیون سلسله مراتبی بین پنج ویژگی شخصیتی (روانرنجورخویی، برونگرایی، گشودگی به



تجربه، توافقجویی و مسئولیتپذیری) و سه نوع همسرآزاری علیه زنان (خشونت روانشناختی، خشونت جسمانی و خشونت جنسی) استفاده شد. متغیر وابسته نمرات نشانگان افسردگی است.
چنانکه در جدول شماره 2 مشاهده میشود، در گام اول رگرسیون سلسله مراتبی، متغیر مستقل (خشونت روانشناختی) وارد معادله شده است. در این حالت ضریب رگرسیون بهدستآمده معنادار است (376/0=B، 01/0≥ P)؛ یعنی خشونت روانشناختی علیه زنان میتواند بروز نشانههای افسردگی را به میزان زیادی
چنانکه در جدول شماره 2 مشاهده میشود، در گام اول رگرسیون سلسله مراتبی، متغیر مستقل (خشونت روانشناختی) وارد معادله شده است. در این حالت ضریب رگرسیون بهدستآمده معنادار است (376/0=B، 01/0≥ P)؛ یعنی خشونت روانشناختی علیه زنان میتواند بروز نشانههای افسردگی را به میزان زیادی


پیشبینی کند. در گام دوم متغیر تعدیلکننده (ویژگی شخصیتی توافقجویی) وارد معادله شده است که در این حالت ضریب رگرسیون معنادار است (182/0-=B، 01/0≥P)؛ یعنی ویژگی شخصیتی توافقجویی در فرد میتواند نمرات نشانگان افسردگی او را پیشبینی کند. در گام سوم نیز تعامل متغیر مستقل و تعدیلکننده وارد شدهاند که ضریب رگرسیون در این صورت نیز معنادار است (155/0-=B، 05/0≥P). یعنی ویژگی شخصیتی توافقجویی در رابطه بین خشونت (همسرآزاری) روانشناختی و نمرات نشانگان افسردگی اثر تعدیلکنندگی دارد. در خصوص خشونت جنسی نیز همانطور که در جدول مشاهده میشود (125/0-=B، 05/0≥P)، ضریب رگرسیون معنادار است؛ یعنی ویژگی شخصیتی توافقجویی در رابطه میان همسرآزاری جنسی و افسردگی نقش تعدیلکنندگی دارد. نقاط مورد نیاز برای ترسیم نمودار رگرسیون در جدول شماره 3 وارد شده است.
چنان که در تصویر شماره 1 مشاهده میشود، بدیهی است افرادی که به میزان بیشتری توافقجو هستند، در مقایسه با افرادی که این ویژگی را به میزان متوسط و کم دارند، کمتر نشانههای افسردگی را بروز میدهند؛ اما زمانی که میزان خشونت روانشناختی کم باشد، تفاوت این سه گروه ناچیز است. هرچه میزان همسرآزاری روانشناختی افزایش یابد، تفاوت این سه گروه بیشتر میشود. در تفاوت شیب سه نمودار هم هرچه افراد کمتر توافقجو باشند، میزان همسرآزاری روانشناختیای که بر آنها وارد میشود، بیشتر میتواند میزان نشانههای افسردگی آنها را تعیین کند.
افرادی که به میزان بیشتری توافقجو هستند، در مقایسه با افرادی که این ویژگی را به میزان متوسط و کم دارند، کمتر نشانگان افسردگی را بروز میدهند؛ اما زمانی که میزان خشونت جنسی کم باشد، تفاوت بین این سه گروه ناچیز است. هرچه میزان همسرآزاری جنسی افزایش یابد، تفاوت این سه گروه بیشتر میشود. درباره تفاوت شیب سه نمودار هم باید اذعان داشت که هرچه افراد کمتر توافقجو باشند، میزان همسرآزاری جنسی بیشتر میتواند میزان نشانه های افسردگی آنها را پیشبینی کند (تصویر شماره 2).
بحث
نتایج بررسی های انجام شده در این پژوهش، از ارتباط مستقیم میان همسرآزاری علیه زنان و نشانگان افسردگی در آن ها حمایت میکند. به عبارت دیگر، زنانی که دچار همسرآزاری میشوند، به طور معناداری دچار نشانههای افسردگی هستند. پژوهشهای پیشین نیز حاکی از آن است که زنانی که همسرانشان نسبت به آنها خشونت دارند، بیشتر از زنان دیگر افسرده هستند [31 ،19 ،16].
این یافته با استفاده از نظریه سندروم زنان کتکخورده والکر [37] که بر پایه نظریه درمانگی آموختهشده سلیگمن بنا شده، قابل تبیین است. والکر زنان قربانی همسرآزاری را مبتلا به «سندروم زنان کتک خورده« میداند. وی این سندروم را با استفاده از اصطلاحات تشخیصی اینگونه تعریف کرده است: «رشد علائم و ناهنجاریهای جسمانی، روانشناختی و اجتماعی مانند افسردگی، عزت نفس کم و انزوا که به دنبال تجربه خشونت از سوی همسر رخ میدهد.» [37] به اعتقاد والکر، زنان خشونتدیده با گذشت زمان و تکرار دورههای کنترلنشدنی و پیشبینیناپذیر خشونت، متوجه میشوند که اعمال آنها هیچ تغییری در رابطه ایجاد نکرده است [38] و احساس کنترل خود بر موقعیتهای تنشزا را از دست میدهند؛ در نتیجه برای ترک فرد خشونتگر احساس درماندگی میکنند و این موضوع موجب افسردگی آنها میشود [39].
بر اساس یافتههای پژوهش حاضر، افرادی که به میزان بیشتری توافقجو هستند، به طور کلی در مقایسه با افرادی که این ویژگی را به میزان متوسط و کم دارند، کمتر نشانههای افسردگی را بروز میدهند. زمانی که میزان خشونت روانشناختی کم باشد، تفاوت این سه گروه ناچیز است. هرچه میزان همسرآزاری روانشناختی و جنسی افزایش یابد، تفاوت این سه گروه بیشتر میشود. به عبارت دیگر، هر چه افراد کمتر توافقجو باشند، میزان همسرآزاری روانشناختیای که بر آنها وارد میشود، بیشتر میتواند میزان نشانههای افسردگی آنها را تعیین کند.
بر اساس یافتههای پژوهش شوت و همکاران (2014) ویژگی شخصیتی توافقجویی با انتقاد از خود و نمرات افسردگی ارتباط منفی معناداری دارد. در همین راستا فینچ و گرازیانو [40] در پژوهش خود نشان دادند ویژگی شخصیتی توافقجویی به صورت غیرمستقیم با افسردگی در ارتباط است. افراد توافقجو، دوستان بیشتری دارند، حمایت اجتماعی بیشتری دریافت میکنند و مقابلههای مؤثرتری به کار میبرند که تمامی اینها با احتمال افسردگی کمتر مرتبط است [41].
برای تبیین این یافتهها میتوان از ویژگیهای سازه توافقجویی استفاده کرد. افرادی که به میزان زیادی این ویژگی را دارند، در روابط بین فردی معتمد، خوشبین و همکار هستند. آنها افرادی مؤدب، گرم، دوستداشتنی، انعطافپذیر، بخشنده، ملایم، دلسوز، باملاحظه و منطقی هستند. این افراد تمایل بسیاری برای کمک به دیگران دارند و به آنها با دیدی مثبت مینگرند [42]. به علاوه افراد توافقجو، رفتارهای اجتماعی دیگران را کمتر ستیزهجویانه تفسیر میکنند و بیشتر تمایل دارند در روابط اجتماعی که صمیمیت را تسهیل میکند، درگیر شوند [43]. این ویژگیها و داشتن دیدی مثبت به افراد و حوادث موجب میشود که زنان قربانی همسرآزاری توافقجو در مقایسه با دیگران کمتر دچار افسردگی شوند.
نتیجهگیری
به طورکلی پژوهش حاضر نشان داد زنانی که دچار همسرآزاری میشوند، به طور معناداری بیشتر در معرض افسردهشدن قرار دارند و قربانیانی که توافقجوتر هستند، نشانههای افسردگی کمتری خواهند داشت.
استفاده از پرسشنامههای خودگزارشی موجب افزایش احتمال پاسخدهی ذهنی و بیصداقتی شرکتکنندگان در پاسخدادن به سؤالات پرسشنامهها میشود. به علاوه در پرسشنامه همسرآزاری، تعدادی از سؤالات خشونت جنسی را بررسی میکنند که به علت مقاومت شرکتکنندگان در پاسخدهی، احتمال صداقت نداشتن و سوگیری وجود دارد. روش نمونهگیری در پژوهش حاضر در دسترس است؛ لذا تعمیم یافتههای پژوهش به کل جامعه با قطعیت ممکن نیست.
در پژوهش حاضر به بررسی نقش متغیرهای فردی در روابط خشونتبار زوجها پرداخته شده است. در حالی که یکی از متغیرهای اصلی در این حوزه رابطه زوجهاست. پیشنهاد می شود پژوهشگران آتی به بررسی این عامل مهم در روابط خشونتآمیز زوجها بپردازند. همچنین پیشنهاد میشود در مطالعات آینده نقش عوامل دموگرافیک نظیر وجود فرزند، مدت ازدواج و مرحله چرخه زندگی بررسی شود.
سپاسگزاری
بدینوسیله از معاونت پژوهشی و پژوهشکده خانواده دانشگاه شهید بهشتی که از این پژوهش حمایت مالی کردند، قدردانی میشود. این مقاله برگرفته از پایاننامه کارشناسی ارشد نویسنده اول است. بنا به اظهار نویسنده مسئول مقاله، تعارض منافع وجود نداشته است.
چنان که در تصویر شماره 1 مشاهده میشود، بدیهی است افرادی که به میزان بیشتری توافقجو هستند، در مقایسه با افرادی که این ویژگی را به میزان متوسط و کم دارند، کمتر نشانههای افسردگی را بروز میدهند؛ اما زمانی که میزان خشونت روانشناختی کم باشد، تفاوت این سه گروه ناچیز است. هرچه میزان همسرآزاری روانشناختی افزایش یابد، تفاوت این سه گروه بیشتر میشود. در تفاوت شیب سه نمودار هم هرچه افراد کمتر توافقجو باشند، میزان همسرآزاری روانشناختیای که بر آنها وارد میشود، بیشتر میتواند میزان نشانههای افسردگی آنها را تعیین کند.
افرادی که به میزان بیشتری توافقجو هستند، در مقایسه با افرادی که این ویژگی را به میزان متوسط و کم دارند، کمتر نشانگان افسردگی را بروز میدهند؛ اما زمانی که میزان خشونت جنسی کم باشد، تفاوت بین این سه گروه ناچیز است. هرچه میزان همسرآزاری جنسی افزایش یابد، تفاوت این سه گروه بیشتر میشود. درباره تفاوت شیب سه نمودار هم باید اذعان داشت که هرچه افراد کمتر توافقجو باشند، میزان همسرآزاری جنسی بیشتر میتواند میزان نشانه های افسردگی آنها را پیشبینی کند (تصویر شماره 2).
بحث
نتایج بررسی های انجام شده در این پژوهش، از ارتباط مستقیم میان همسرآزاری علیه زنان و نشانگان افسردگی در آن ها حمایت میکند. به عبارت دیگر، زنانی که دچار همسرآزاری میشوند، به طور معناداری دچار نشانههای افسردگی هستند. پژوهشهای پیشین نیز حاکی از آن است که زنانی که همسرانشان نسبت به آنها خشونت دارند، بیشتر از زنان دیگر افسرده هستند [31 ،19 ،16].
این یافته با استفاده از نظریه سندروم زنان کتکخورده والکر [37] که بر پایه نظریه درمانگی آموختهشده سلیگمن بنا شده، قابل تبیین است. والکر زنان قربانی همسرآزاری را مبتلا به «سندروم زنان کتک خورده« میداند. وی این سندروم را با استفاده از اصطلاحات تشخیصی اینگونه تعریف کرده است: «رشد علائم و ناهنجاریهای جسمانی، روانشناختی و اجتماعی مانند افسردگی، عزت نفس کم و انزوا که به دنبال تجربه خشونت از سوی همسر رخ میدهد.» [37] به اعتقاد والکر، زنان خشونتدیده با گذشت زمان و تکرار دورههای کنترلنشدنی و پیشبینیناپذیر خشونت، متوجه میشوند که اعمال آنها هیچ تغییری در رابطه ایجاد نکرده است [38] و احساس کنترل خود بر موقعیتهای تنشزا را از دست میدهند؛ در نتیجه برای ترک فرد خشونتگر احساس درماندگی میکنند و این موضوع موجب افسردگی آنها میشود [39].
بر اساس یافتههای پژوهش حاضر، افرادی که به میزان بیشتری توافقجو هستند، به طور کلی در مقایسه با افرادی که این ویژگی را به میزان متوسط و کم دارند، کمتر نشانههای افسردگی را بروز میدهند. زمانی که میزان خشونت روانشناختی کم باشد، تفاوت این سه گروه ناچیز است. هرچه میزان همسرآزاری روانشناختی و جنسی افزایش یابد، تفاوت این سه گروه بیشتر میشود. به عبارت دیگر، هر چه افراد کمتر توافقجو باشند، میزان همسرآزاری روانشناختیای که بر آنها وارد میشود، بیشتر میتواند میزان نشانههای افسردگی آنها را تعیین کند.
بر اساس یافتههای پژوهش شوت و همکاران (2014) ویژگی شخصیتی توافقجویی با انتقاد از خود و نمرات افسردگی ارتباط منفی معناداری دارد. در همین راستا فینچ و گرازیانو [40] در پژوهش خود نشان دادند ویژگی شخصیتی توافقجویی به صورت غیرمستقیم با افسردگی در ارتباط است. افراد توافقجو، دوستان بیشتری دارند، حمایت اجتماعی بیشتری دریافت میکنند و مقابلههای مؤثرتری به کار میبرند که تمامی اینها با احتمال افسردگی کمتر مرتبط است [41].
برای تبیین این یافتهها میتوان از ویژگیهای سازه توافقجویی استفاده کرد. افرادی که به میزان زیادی این ویژگی را دارند، در روابط بین فردی معتمد، خوشبین و همکار هستند. آنها افرادی مؤدب، گرم، دوستداشتنی، انعطافپذیر، بخشنده، ملایم، دلسوز، باملاحظه و منطقی هستند. این افراد تمایل بسیاری برای کمک به دیگران دارند و به آنها با دیدی مثبت مینگرند [42]. به علاوه افراد توافقجو، رفتارهای اجتماعی دیگران را کمتر ستیزهجویانه تفسیر میکنند و بیشتر تمایل دارند در روابط اجتماعی که صمیمیت را تسهیل میکند، درگیر شوند [43]. این ویژگیها و داشتن دیدی مثبت به افراد و حوادث موجب میشود که زنان قربانی همسرآزاری توافقجو در مقایسه با دیگران کمتر دچار افسردگی شوند.
نتیجهگیری
به طورکلی پژوهش حاضر نشان داد زنانی که دچار همسرآزاری میشوند، به طور معناداری بیشتر در معرض افسردهشدن قرار دارند و قربانیانی که توافقجوتر هستند، نشانههای افسردگی کمتری خواهند داشت.
استفاده از پرسشنامههای خودگزارشی موجب افزایش احتمال پاسخدهی ذهنی و بیصداقتی شرکتکنندگان در پاسخدادن به سؤالات پرسشنامهها میشود. به علاوه در پرسشنامه همسرآزاری، تعدادی از سؤالات خشونت جنسی را بررسی میکنند که به علت مقاومت شرکتکنندگان در پاسخدهی، احتمال صداقت نداشتن و سوگیری وجود دارد. روش نمونهگیری در پژوهش حاضر در دسترس است؛ لذا تعمیم یافتههای پژوهش به کل جامعه با قطعیت ممکن نیست.
در پژوهش حاضر به بررسی نقش متغیرهای فردی در روابط خشونتبار زوجها پرداخته شده است. در حالی که یکی از متغیرهای اصلی در این حوزه رابطه زوجهاست. پیشنهاد می شود پژوهشگران آتی به بررسی این عامل مهم در روابط خشونتآمیز زوجها بپردازند. همچنین پیشنهاد میشود در مطالعات آینده نقش عوامل دموگرافیک نظیر وجود فرزند، مدت ازدواج و مرحله چرخه زندگی بررسی شود.
سپاسگزاری
بدینوسیله از معاونت پژوهشی و پژوهشکده خانواده دانشگاه شهید بهشتی که از این پژوهش حمایت مالی کردند، قدردانی میشود. این مقاله برگرفته از پایاننامه کارشناسی ارشد نویسنده اول است. بنا به اظهار نویسنده مسئول مقاله، تعارض منافع وجود نداشته است.
References
[1]Kalaca S, Dundar P. Violence against women: The perspective of academic women. BMC Public Health. 2010; 10(1):490. doi: 10.1186/1471-2458-10-490
[2]Meier JS. Brief of the domestic violence legal empowerment and appeals project, aequitas: The prosecutors’ resource on violence against women, & futures without violence as Amici Curiae in support of respondent, Voisine v (Report). Report No. 14-10154. Washington D. C.: GW Law Faculty Publication; 2016.
[3]Tjaden PG, Thoennes N. Extent, nature, and consequences of intimate partner violence: Findings from the National Violence Against Women Survey. Washington D. C.: National Institute of Justice; 2000.
[4]Krantz G, van Phuong T, Larsson V, Thuan NT, Ringsberg KC. Intimate partner violence: Forms, consequences and preparedness to act as perceived by healthcare staff and district and community leaders in a rural district in northern Vietnam. Public Health. 2005; 119(11):1048-55. doi: 10.1016/j.puhe.2005.03.015
[5]Walker LE. Psychology and domestic violence around the world. American Psychologist. 1999; 54(1):21-29. doi: 10.1037//0003-066x.54.1.21
[6]Amoakohene MI. Violence against women in Ghana: A look at women’s perceptions and review of policy and social responses. Social Science & Medicine. 2004; 59(11):2373-85. doi: 10.1016/j.socscimed.2004.04.001
[7]Women‘s Research and Studies Center. Preventing Violence against women and children: Workshop summary. New York: National Academies Press; 2001.
[8]Abbott J, Johnson R, Koziol-McLain J, Lowenstein SR. Domestic violence against women: Incidence and prevalence in an emerg ency department population. Journal of the American Medical Association. 1995; 273(22):1763-7. doi: 10.1001/jama.273.22.1763
[9]Campbell JC, Lewandowski LA. Mental and physical health effects of intimate partner violence on women and children. Psychiatric Clinics of North America. 1997; 20(2):353-74. doi: 10.1016/s0193-953x(05)70317-8
[10]Dienemann J, Boyle E, Baker D, Resnick W, Wiederhorn N, Campbell J. Intimate partner abuse among women diagnosed with depression. Issues in Mental Health Nursing. 2000; 21(5):499-513. doi: 10.1080/01612840050044258
[11]Jones L, Hughes M, Unterstaller U. Post-Traumatic Stress Disorder (PTSD) in victims of domestic violence: A review of the research. Trauma, Violence, & Abuse. 2001; 2(2):99-119. doi: 10.1177/1524838001002002001
[12]Stein MB, Kennedy C. Major depressive and post-traumatic stress disorder comorbidity in female victims of intimate partner violence. Journal of Affective Disorders. 2001; 66(2-3):133-8. doi: 10.1016/s0165-0327(00)00301-3
[13]Straus MA, Gelles RJ, Smith C. Physical violence in American families: Risk factors and adaptations to violence in 8,145 families. New Brunswick, NJ: Transaction Publishers; 1990.
[14]Hilberman E, Munson K. Sixty battered women. Victimology. 1977; 2(3-4): 460-470.
[15]Bonomi AE, Anderson ML, Reid RJ, Rivara FP, Carrell D, Thompson RS. Medical and psychosocial diagnoses in women with a history of intimate partner violence. Archives of Internal Medicine. 2009; 169(18):1692-7. doi: 10.1001/archinternmed.2009.292
[16]Tsai AC, Tomlinson M, Comulada WS, Rotheram-Borus MJ. Intimate partner violence and depression symptom severity among South African women during pregnancy and postpartum: Population-based prospective cohort study. PLOS Medicine. 2016; 13(1):1001943. doi: 10.1371/journal.pmed.1001943
[17]Golding JM. Intimate partner violence as a risk factor for mental disorders: A meta-analysis. Journal of Family Violence. 1999; 14(2):99-132. doi: 10.1023/A:1022079418229
[18]Mapayi B, Makanjuola RO, Mosaku SK, Adewuya OA, Afolabi O, Aloba OO, et al. Impact of intimate partner violence on anxiety and depression amongst women in Ile-Ife, Nigeria. Archives of Women's Mental Health. 2013; 16(1):11-8. doi: 10.1007/s00737-012-0307-x
[19]Wong J, Mellor D. Intimate partner violence and women’s health and wellbeing: Impacts, risk factors and responses. Contemporary Nurse. 2014; 46(2):170-9. doi: 10.5172/conu.2014.46.2.170
[20]Estefan LF, Coulter ML, VandeWeerd C. Depression in women who have left violent relationships: The unique impact of frequent emotional abuse. Violence Against Women. 2016; 12(11): 1397 to 1413. doi: 10.1177/1077801215624792
[21]Davins-Pujols M, Pérez-Testor C, Salamero-Baró M, Castillo-Garayoa JA. Personality profiles in abused women receiving psychotherapy according to the existence of childhood abuse. Journal of Family Violence. 2012; 27(2):87-96. doi: 10.1007/s10896-011-9407-z
[22]Torres A, Garcia-Esteve L, Navarro P, Tarragona MJ, Imaz ML, Ascaso C, et al. Relationship between intimate partner violence, depressive symptomatology, and personality traits. Journal of Family Violence. 2013; 28(4):369-79. doi: 10.1007/s10896-013-9502-4
[23]Gellen MI, Hoffman RA, Jones M, Stone M. Abused and nonabused women: MMPI profile differences. The Personnel and Guidance Journal. 1984; 62(10):601-4. doi: 10.1111/j.2164-4918.1984.tb00134.x
[24]Jang KL, Stein MB, Taylor S, Asmundson GJ, Livesley WJ. Exposure to traumatic events and experiences: aetiological relationships with personality function. Psychiatry Research. 2003; 120(1):61-9. doi: 10.1016/s0165-1781(03)00172-0
[25]Löckenhoff CE, Terracciano A, Patriciu NS, Eaton WW, Costa PT. Self‐reported extremely adverse life events and longitudinal changes in five‐factor model personality traits in an urban sample. Journal of Traumatic Stress. 2009; 22(1):53-9. doi: 10.1002/jts.20385
[26]Motevaliyan SM, Yaacob SN, Juhari R, Mansor M, Dokoushkani F, Watson PJ. Associations of personality traits and childhood insult experience with perceived husbands’ psychological aggression among Iranian women. Journal of Family Violence. 2016. doi: 10.1007/s10896-016-9811-5
[27]Estrellado AF. Assessing the personality profile of battered women. In: Faulkner AG, editor. The Assessment Handbook. Coleraine: Ulster University; 2010.
[28]Yaghubkhani Ghiasvand M, Fathi Aghdam G. [Personality correlates of emotionally abused students with opposite sex (Persian)]. Journal of Qazvin University of Medical Sciences. 2012; 16(3):61-65.
[29]Panaghi L, Pirouzi D, Shirinbayan M, Ahmadi Z. [The role of personality and demographic traits in spouse abuse (Persian)].Iranian Journal of Psychiatry and Clinical Psychology. 2011; 17(2):126-135.
[30]Ghahari SH, Atefvahid MK, Yousefi H. [The prevalence of spouse abuse among married students of Islamic Azad University of Tonekabon in 2004 (Persian)]. Journal of Mazandaran University of Medical Sciences. 2006; 15(50):83-89.
[31]Dasarband B. [The moderating role of personality characteristics and stress coping strategies in the relation between spouse abuse with women’s depressive symptoms and couple burnout (Persian)] [MA thesis]. Tehran: Shahid Beheshti University; 2015.
[32]Stefan-Dabson K, Mohammadkhani P, Massah-Choulabi O. [Psychometrics characteristic of Beck depression Inventory-II in patients with major depressive disorder (Persian)]. Journal of Rehabilitation. 2007; 8:80-86.
[33]Fata L, Birshak B, Atefvahid MK, Dabson KS. [Meaning assignment structure/ schema, emotional states and cognitive processing of emotional information: Comparing two conceptual frameworks (Persian)]. Iranian Journal of Psychiatry and Clinical Psychology. 2005; 11(3):312-326.
[34]Roshan Chosli R, Shaeiri M, Atri Fard M, Nikkhah A, Ghaem Maghami B, Rahimi Rad A. [Investigating psychometric properties of “NEO-Five Factor Inventory” (NEO-FFI) (Persian)]. Daneshvar Raftar. 2006; 13(16):27-36.
[35]Aliloo MM, Arji A, Bakhshipoor Rudsari A, Shahjui T. [The relation between personality and coping strategies in drug users with HIV (Persian)]. Medical Journal of Tabriz University of Medical Sciences & Health Services. 2009; 1(33):70-76.
[36]Barnett OW. Why battered women do not leave, Part 2 external inhibiting factors—social support and internal inhibiting factors. Trauma, Violence, & Abuse. 2001; 2(1):3-35. doi: 10.1177/1524838001002001001
[37]Walker LE. Psychology and domestic violence around the world. American Psychologist. 1999; 54(1):21-29. doi: 10.1037//0003-066x.54.1.21
[38]Miller JB. The development of women’s sense of self. In: Jordan JV, Kaplan AG, Stiver IP, Surrey JL, Baker Miller J, editors. Women’s Growth in Connection: Writings from the Stone Center. New York: Guilford Press; 1991.
[39]Craven Z. Battered woman syndrome. Australian Domestic & Family Violence Clearinghouse; Philadelphia: Sage; 2003.
[40]Finch JF, Graziano WG. Predicting depression from temperament, personality, and patterns of social relations. Journal of Personality. 2001; 69(1):27-55. doi: 10.1111/1467-6494.00135
[41]van Straten A, Cuijpers P, van Zuuren FJ, Smits N, Donker M. Personality traits and health-related quality of life in patients with mood and anxiety disorders. Quality of Life Research. 2006; 16(1):1-8. doi: 10.1007/s11136-006-9124-x
[42]Costa PT, McCrae RR. Neo PI/FFI manual supplement. Odessa, FL: Psychological Assessment Resources. 1989.
[43]Graziano WG, Jensen-Campbell LA, Hair EC. Perceiving interpersonal conflict and reacting to it: the case for agreeableness. Journal of Personality and Social Psychology. 1996; 70(4):820-835. doi: 10.1037//0022-3514.70.4.820
Type of Study: Original Research |
Subject:
Psychiatry and Psychology
Received: 2016/09/3 | Accepted: 2017/01/21 | Published: 2017/04/1
Received: 2016/09/3 | Accepted: 2017/01/21 | Published: 2017/04/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
